PMA’s core survey collects data across selected geographies to track indicators of family planning demand, access, and use on an annual basis at both household and health facility levels to inform policies and programs. Its data collection design introduced an innovative approach by recruiting women from their communities who are trained to collect data using smartphone technology.
Building upon this innovative design, PMA has continued innovating in numerous ways with modifications to design and content that advance our understanding of contraceptive use dynamics, as well other areas of public health. Listed below are examples of these innovations with links to publications that provide more detail.

COVID-19
PMA quickly pivoted to address the COVID-19 pandemic by administering a survey measuring media exposure to COVID-19 messages, perceived risk of infection, behavior change, the economic impact, and the impact of COVID-19 on family planning-related outcomes. The PMA COVID-19 survey results have been provided to local governments to produce actionable information and guide the public health response to COVID-19.

PMA Ethiopia
Maternal and newborn health (MNH) was evaluated through two survey projects in Ethiopia to generate new information on key maternal and newborn health indicators. The PMA Maternal and Newborn Health (MNH) Survey launched in 2016 in Southern Nations, Nationalities and Peoples’ region (SNNPR), and was designed to collect information on knowledge, practice and coverage of MNH services. Its successor, PMA-Ethiopia, launched in 2019, implementing cross-sectional, longitudinal, and facility-based surveys with a focus on measuring the comprehensiveness of RMNH care services and the barriers and facilitators to such care. Read more here.
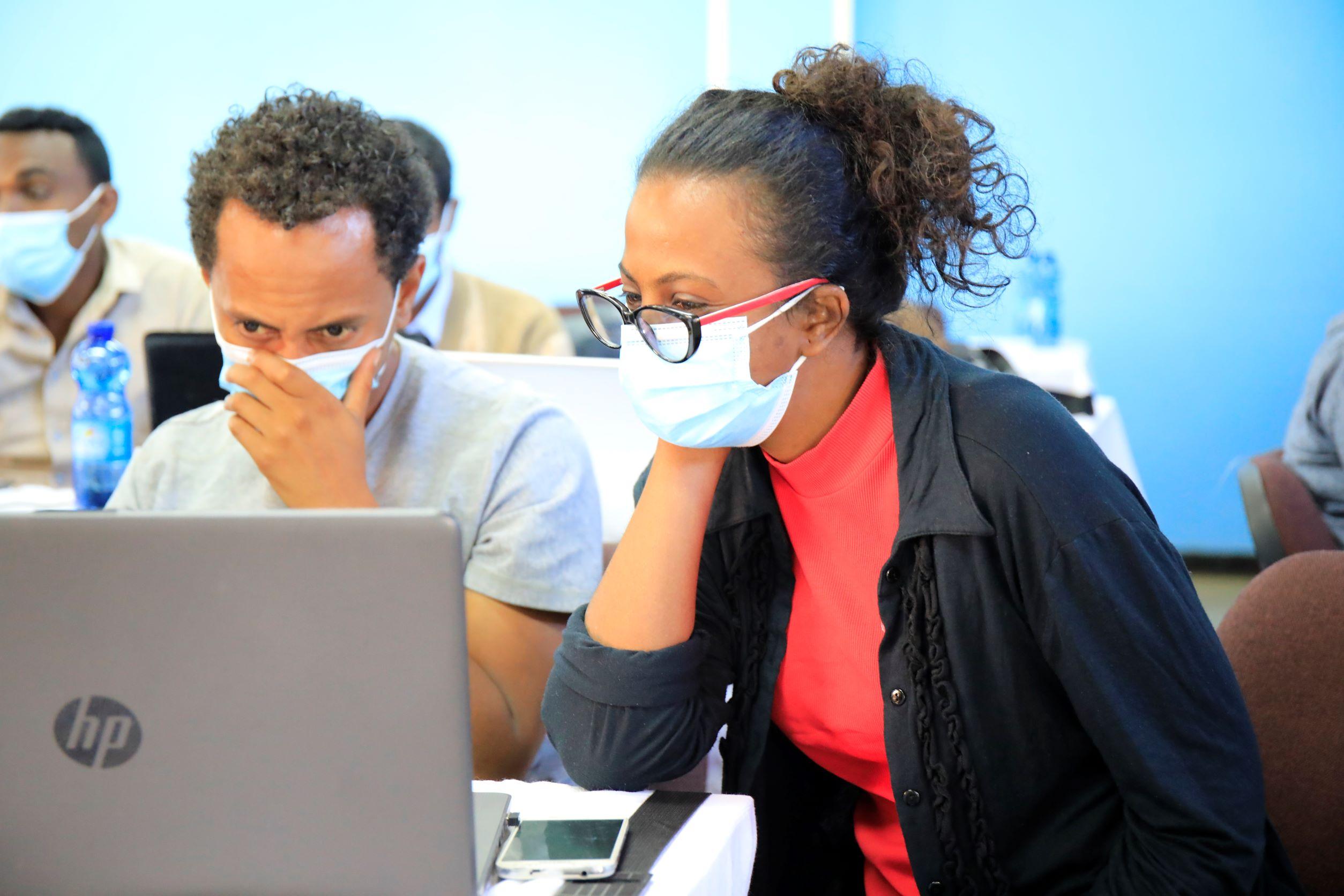
Data Analysis Course
PMA Ethiopia held a data analysis course with Addis Ababa University and regional universities to help academic researchers build their knowledge and skills related to advanced statistical research techniques. The course also covered large-scale survey design and manuscript development training. Course participants work in groups with support from Johns Hopkins Bloomberg School of Health faculty and students to complete academic journal manuscripts based on analyses of PMA Ethiopia data.

PMA Ethiopia Mentorship Program
Through the PMA Ethiopia research mentorship program, faculty at the Johns Hopkins Bloomberg School of Public Health provides mentorship to Ph.D. students and junior faculty at Addis Ababa University and regional universities as they complete public health research using PMA Ethiopia data. Ph.D. students are enrolled in the program through the completion of their dissertation and junior faculty are enrolled through the completion of two to three academic journal manuscripts. The program also supports mentees to take Johns Hopkins University coursework.

Longitudinal Panel Data
Longitudinal panel data demonstrates the value of measuring background/demand information at baseline as leading indicators for contraception adoption/continuation -- and incorporating questions in areas that will be used in future surveys, including women’s agency and community norms.

Women & Girls’ Empowerment
Women & girls’ empowerment is studied across all PMA countries, with a focus on sexual, reproductive, and economic empowerment. This started with a qualitative study that led to the development of several measures of these concepts, which are now incorporated into PMA panel data collection. Read the executive summary of this study here and the complete study here.

DMPA-SC and Self-Injection
PMA has been tracking use of DMPA-SC since its introduction in each PMA country, and has recently added measures of self-injection of DMPA-SC, along with knowledge of and attitudes towards DMPA-SC. Some of our recent work can be found here.
Abortion Modules
Abortion modules introduced in three countries (Cote d’Ivoire, India, Nigeria) demonstrate the value of encompassing a “confidante” measure that better estimates true abortion rates. Components have also been incorporated to better understand factors underlying decisions and methods used and to better understand medical abortion availability. Briefs are available from Cote d’Ivoire, India, and Nigeria.

Client-Exit Interviews (CEIs)
PMA collects information from family planning clients at health facilities in the PMA sample, and follows up with these clients six months later. Measures in client exit interviews baseline and follow-up surveys include: quality of care indicators for family planning services and contraceptive counseling, user experience with current method, as well as contraceptive use, discontinuation, and future use. These data are also provided quickly for use by data managers through dashboards, such as this one from Kenya. Results from these interviews are summarized in briefs, such as these from Nigeria Ogun State, Kericho Kenya, and Kinshasa DRC.

Gender-Based Violence
Given the potential for COVID-19 restrictions to increase gender-based violence (GBV), countries could opt-in to a GBV mini-module beginning to 2020. The mini-module includes questions on prevalence and intensity of intimate partner violence (IPV) and household violence, as well as help-seeking behaviors. PMA Ethiopia additionally assesses IPV during pregnancy and YRDS examines IPV and non-partner sexual assault for urban adolescents. Reproductive coercion, a type of IPV where partners interfere in women’s contraceptive use, is assessed across PMA, PMA Ethiopia, and YRDS. View our survey results here.

Youth Respondent Driven Sampling (YRDS)
Youth Respondent Driven Sampling (YRDS) approach was implemented in Abidjan and Nairobi with sexually-active, unmarried female and male youth to better capture contraceptive access, norms and “hidden” use dynamics, including coercion, in a population that is often under-and misrepresented with traditional survey designs. Read more about YRDS in Abidjan and Nairobi.

Quarterly Facility Surveys
Quarterly facility surveys provide information, via our recently concluded PMA Agile project, on contraceptive method availability, stock-outs, and volumes of clients served, shared with public and private program managers through rapidly posted dashboards, such as this one from Kenya. Data are also shared through briefs, such as these from Nigeria Ogun State, Kericho Kenya, and Kinshasa DRC.

Implant Use and Removal
Implant Use and Removal questions are added to survey rounds in countries with high implant use. The questions encompass background characteristics of implant users, service readiness to remove implants, counseling on removal, and implant removal experience among women who have sought but not received a removal. Read the results from Ethiopia here.

Nutrition
Nutrition data was collected in Burkina Faso and Kenya over two rounds, covering interventions received during antenatal care visits, breastfeeding and complementary feeding practices, receipt of under-5 interventions, dietary practices among key sub-populations, and food security. Read more about nutrition findings in Burkina Faso and Kenya. A report on technical innovations was also produced that included questions about coverage of nutrition-specific interventions and diet that are not commonly measured in nationally representative household surveys.

Primary Health Care
Primary Health Care information was collected in Ghana and more recently in Uganda under a collaboration with Harvard University, Ariadne Labs. The Uganda survey revealed that most people report significant financial barriers to access care, that most lack continuous relationships with a care provider, while providers lack access to patient information. Read more here.

Water and Sanitation/Schistosomiasis
Water and Sanitation/Schistosomiasis monitoring was supported in Uganda over two rounds of nation-level data collection that revealed higher levels of prevalence than expected among all educational levels and wealth quintiles. Children ages 2-4 are the most at-risk age group for schistosomiasis. Read more here.

Menstrual Hygiene Management (MHM)
Menstrual Hygiene Management (MHM) modules were included in 12 PMA survey rounds and encompassed questions on the type of MHM materials used, location for changing materials and the safety, cleanliness and privacy of these locations. Read more MHM findings for Niger, Ethiopia, and Kongo Central DRC.

Exposure to Communication Interventions
Exposure to family planning communication interventions was evaluated in DRC from 2016-2018, through a collaboration with the Johns Hopkins Center for Communication Programs. PMA data are cited in CCP’s Family Planning and the ‘Voice of Youth’ in Democratic Republic of Congo.